EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic)
EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic) •
EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic) •• EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic) • • EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic) • • EU Warehouse V1 shipping to USA (HT‑PHARM, Proper, Pharmaqo) is paused. Choose Beligas (USA Domestic) ••
Blog
Home » Blog » SARMs vs Steroids: Understanding the Differences and Making the Right Choice
Disclaimer: The following article is for educational purposes only and does not promote the use of illegal substances. Only researchers are authorized to administer SARMs, as they are not FDA-approved for cosmetic use and may have adverse effects. Dr. Grant F. is available for consultation should readers have any questions or concerns.
The debate between selective androgen receptor modulators (SARMs) and anabolic-androgenic steroids (AAS) continues to intensify as more individuals seek performance-enhancing compounds. Both categories of substances offer muscle-building and strength-enhancing properties, yet they differ significantly in their mechanisms of action, side effect profiles, and legal status.
Understanding these differences is crucial for anyone considering either option, as the choice between SARMs and steroids can dramatically impact both results and health outcomes.
What Are SARMs?
Selective androgen receptor modulators are a class of compounds designed to selectively target androgen receptors in specific tissues, primarily muscle and bone. Unlike anabolic steroids, SARMs were formulated to provide the anabolic benefits of androgens whilst minimising unwanted side effects.
The most commonly researched SARMs include:
Ostarine (MK-2866)
RAD-140 (Testolone)
LGD-4033 (Ligandrol)
S23
Andarine (S4)
SARMs work by binding to androgen receptors with tissue selectivity, theoretically allowing them to promote muscle growth and bone density without significantly affecting other organs such as the prostate or liver.
What Are Anabolic Steroids?
Anabolic-androgenic steroids are synthetic derivatives of testosterone that have been used for decades in both medical and performance-enhancing contexts. These compounds affect multiple tissues throughout the body, leading to both desired anabolic effects and unwanted androgenic side effects.
Common anabolic steroids include:
Testosterone (various esters)
Dianabol (Methandrostenolone)
Anavar (Oxandrolone)
Deca-Durabolin (Nandrolone Decanoate)
Trenbolone
Steroids function by binding to androgen receptors throughout the body, resulting in increased protein synthesis, nitrogen retention, and enhanced recovery.
Muscle Building: SARMs vs Steroids
Anabolic Steroids: Superior Muscle Growth
In our experience, anabolic steroids consistently produce more significant muscle hypertrophy compared to SARMs. Human trials comparing the anabolic effects of testosterone enanthate versus SARMs found that participants gained 5-7 kg of lean mass with testosterone, whilst SARMs added only 1-1.5 kg over similar timeframes.
A first-time testosterone cycle can result in 15-30 pounds of lean muscle gain when combined with proper training and nutrition. More potent compounds like Dianabol or Trenbolone can produce even more dramatic results.
SARMs: Moderate Muscle Building
SARMs offer more modest muscle-building effects. RAD-140, considered one of the most potent SARMs, typically results in 5-15 pounds of lean muscle gain over an 8-12 week cycle. Ostarine, being milder, usually produces 3-8 pounds of muscle growth.
Whilst SARMs may not match steroids in terms of raw muscle-building potential, they can provide meaningful results with potentially fewer side effects.
Side Effect Profiles
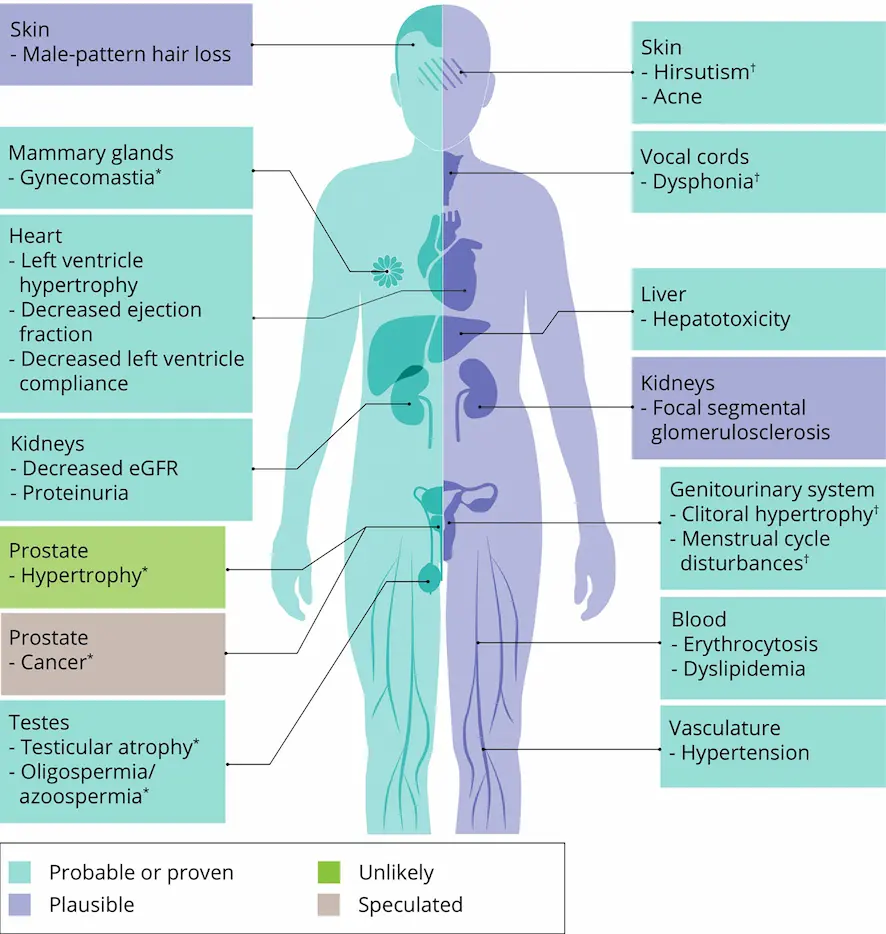
Anabolic Steroids: Comprehensive Impact
Anabolic steroids affect multiple organ systems, leading to a wide range of potential side effects:
Cardiovascular Effects:
Significant alterations in cholesterol levels
Increased blood pressure
Left ventricular hypertrophy
Increased risk of atherosclerosis
Hepatotoxicity:
Oral steroids cause notable liver stress
Elevated liver enzymes (ALT/AST)
Potential for hepatic dysfunction
Hormonal Disruption:
Complete shutdown of natural testosterone production
Testicular atrophy
Gynecomastia (when aromatisation occurs)
Androgenic Effects:
Accelerated male pattern baldness
Acne and oily skin
Prostate enlargement
Virilisation in women
SARMs: Selective but Not Side Effect-Free
Despite claims of tissue selectivity, SARMs are not devoid of adverse effects:
Testosterone Suppression: We have observed significant testosterone suppression with SARMs, particularly with compounds like RAD-140. Users can experience drops from 750 ng/dL to 193 ng/dL after a 12-week cycle.
Hepatotoxicity: Dr. Grant F. has noted that SARMs, including Ostarine and RAD-140, can cause liver stress comparable to taking 50 mg/day of Anavar. Elevated ALT and AST levels are common.
Cardiovascular Impact: Studies show that even mild SARMs like Ostarine can reduce HDL cholesterol by 27%, potentially increasing cardiovascular risk.
Other Effects:
Hair loss (though less common than with steroids)
Potential for gynecomastia
Lipid profile alterations
Legal Status and Availability
Anabolic Steroids
Anabolic steroids are controlled substances in most countries, classified as Schedule III drugs in the United States. They require a prescription for medical use and possession without a prescription is illegal.
SARMs
SARMs occupy a legal grey area. They are not approved by the FDA for human consumption and are banned by WADA for athletic use. However, they are often sold as “research chemicals” online, making them more accessible than traditional steroids.
Detection and Drug Testing
Steroid Detection
Most anabolic steroids can be detected in drug tests for weeks to months after use, depending on the compound and testing method. Detection windows vary significantly:
Testosterone: 2-4 weeks
Nandrolone: Up to 12 months
Stanozolol: 2-6 weeks
SARM Detection
SARMs are increasingly being tested for in competitive sports. Detection times are generally shorter than steroids:
Ostarine: 5-7 days
RAD-140: Estimated 5-10 days
LGD-4033: Similar to Ostarine
Cost Considerations
Anabolic steroids are generally more cost-effective than SARMs. A typical steroid cycle might cost £100-300, whilst a comparable SARM cycle can range from £200-600. This price difference is partly due to SARMs being newer compounds with more complex manufacturing processes.
Post-Cycle Therapy Requirements
Steroids: Comprehensive PCT Needed
Anabolic steroids typically require aggressive post-cycle therapy to restore natural hormone production. A standard PCT protocol might include:
Clomid: 50 mg/day for 4 weeks
Nolvadex: 20 mg/day for 4 weeks
HCG: 2000 IU every other day for 20 days
SARMs: Variable PCT Requirements
SARMs may require less aggressive PCT, though this depends on the compound and dosage used. Mild suppression might only require:
Nolvadex: 20 mg/day for 2-4 weeks
However, potent SARMs like RAD-140 or stacked SARM cycles may require the same comprehensive PCT as steroids.
Results Timeline
Steroids: Rapid Onset
Anabolic steroids typically produce noticeable results within 2-3 weeks of use. Fast-acting compounds like Dianabol can show effects within days.
SARMs: Gradual Progression
SARMs generally require 3-4 weeks before noticeable changes occur. The progression tends to be more gradual and subtle compared to steroids.
Who Should Consider Each Option?
Steroids May Be Appropriate For:
Experienced users who understand the risks
Those seeking maximum muscle growth
Users willing to commit to comprehensive health monitoring
Individuals with access to proper medical oversight
SARMs May Be Suitable For:
Beginners seeking moderate results
Those concerned about androgenic side effects
Users wanting to avoid injection protocols
Individuals seeking specific tissue targeting
Risk-to-Reward Analysis
Both SARMs and steroids carry significant risks that must be weighed against potential benefits. Whilst SARMs were designed to be safer alternatives to steroids, emerging research suggests their side effect profiles may be more similar than initially hoped.
Dr. Grant F. has observed that some SARMs can produce side effects comparable to anabolic steroids, particularly regarding liver toxicity and cardiovascular impact. The notion that SARMs are significantly safer than steroids is increasingly being questioned in clinical practice.
Making an Informed Decision
The choice between SARMs and anabolic steroids should not be taken lightly. Both categories of compounds can produce meaningful changes in body composition, but they also carry substantial health risks.
Key considerations include:
Individual health status and risk tolerance
Experience with performance-enhancing drugs
Access to medical monitoring
Legal implications in your jurisdiction
Long-term health goals versus short-term gains
Neither SARMs nor anabolic steroids should be considered safe for casual use. Both require careful consideration, proper research, and ideally medical supervision.
Conclusion
The comparison between SARMs and anabolic steroids reveals that both categories offer distinct advantages and disadvantages. Whilst steroids generally provide superior muscle-building effects, they come with a more established side effect profile. SARMs, though potentially offering a better side effect profile in theory, are still relatively new compounds with limited long-term safety data.
The decision between these options should be based on individual circumstances, risk tolerance, and thorough understanding of the potential consequences. Regardless of which path one might consider, comprehensive health monitoring and medical oversight remain essential components of any performance-enhancing protocol.
As research continues to evolve, our understanding of both SARMs and steroids will undoubtedly improve, potentially leading to safer and more effective approaches to performance enhancement in the future.