
Testosterone Phenylpropionate – Dosage, PCT, Cycle and Side Effects

Testosterone Phenylpropionate is an anabolic steroid, which is a synthetic form of testosterone hormone that primarily is used for performance enhancement and for testosterone replacement therapy. This has the same effects as the natural hormone, like growth of muscles, increasing red blood cell production, or other regenerative abilities in becoming an overall healthier individual. It’s important to understand the chemical structure of Testosterone Phenylpropionate and its role in the body to help manage use properly and in a healthy manner.
Testosterone Phenylpropionate has specific administration dosages, and using it in conjunction with other steroids has a potentially manageable effect by way of stacking it on a cycle. Testosterone Phenylpropionate will provide a steady release of action therefore promotes stable blood levels. However, the user should be aware the potential side effects, varying from mild to severe; risk management preventative strategies should be of importance. In addition, Post Cycle Therapy (PCT) is a consideration to take into account post cycle Testosterone Phenylpropionate use to restore endogenous testosterone production.
Quick Summary
Testosterone Phenylpropionate is a synthetic hormone which mimics testosterone.
Proper dosing and cycle management is vital to efficacy and safety during use.
Post Cycle Therapy is a significant consideration to HW post use.
Testosterone Phenylpropionate Profile
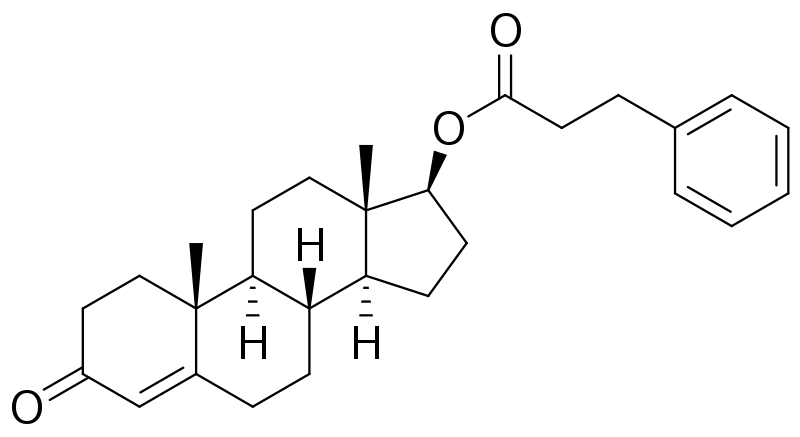
Testosterone Phenylpropionate is an anabolic-androgenic steroid, a synthetic ester, having a phenylpropionate ester attached to the testosterone portion which determines the rate of release and ester half-life. This section will discuss the chemical structure more in-depth, and compare it to testosterone esters.
Chemical Structure and Ester Properties
Testosterone Phenylpropionate is considered to be an estered version of testosterone in that the hormone – testosterone, has an ester, phenylpropionate, that is attached at its beta-hydroxyl group. The presence of this ester has an impact on hormonal lipophilicity and the rate of release from the delivery site into systemic circulation.
Esterification: This enhances the half-life of the medication and offers prolonged release.
Rate of Release: Testosterone Phenylpropionate offers moderate half-life and also moderate relative rate of release, when compared to the propionate ester (which is shorter lived) and cypionate (which is longer lived).
Testosterone Phenylpropionate has a half-life of around 3 to 4.5 days, thus requiring less frequent dosing to maintain stable amounts in the blood as compared to some other esters.
Comparative Half-Lives and Dosing Frequency with other Esters
Testosterone Phenylpropionate is different from other esters in half-life and release profile/duration of action.
Common Testosterone Esters:
| Ester | Half-Life | Injection Frequency |
|---|---|---|
| Testosterone Enanthate | ~4.5-5 days | Every 5-7 days |
| Testosterone Cypionate | ~6-8 days | Every 7-10 days |
| Testosterone Propionate | ~2 days | Every 2-3 days |
| Testosterone Phenylpropionate | ~3-4.5 days | Every 4-6 days |
Differences:
Rate of Release: Rate of release for phenylpropionate is faster than cypionate, but slower than propionate.
Duration: Effects of this ester last longer than testosterone propionate but shorter than enanthate or cypionate esters.
Injection Frequency: Requires more frequency than enanthate or cypionate, but less than propionate, to maintain a stable concentration.
Dosage and Administration

Testosterone phenylpropionate is an injectable form of testosterone that can usually be compared to different injection schemes depending on user experience level (i.e. ease of injection technique). Proper techniques of administration are vital for efficacy and safety.
Suggested Dosage
Beginner: For someone new to using steroids, perhaps a good starting dose could be in the range of 300-500 mg per week. Beginner: People with past steroid experience can go as far as 500 to 700 mg weekly.
Intermediate: A user with experience could do somewhere between 700 to over 1000 mg weekly, however there is a greater risk of side effects and also risk of failure in weaning off.
The actual dosage is user dependant, all users should confirm favorable testosterone levels through lab work via blood tests.
Injection Methods
Dosage Frequency: Due to a half life of around 4 to 5 days, testosterone phenpropionate is best administered at least two times a week to maintain and stabilize blood levels.
Injection Site: User can choose the gluteal mass (butt) or thigh.
User Prep: The injection site should be cleansed with alcohol solution.
Technique: I prefer a thick-gauge needle (22-23 guage) for drawing the solution and switch to a thinner needle (25-27) for injection.
At the injection site, consistency and prophylaxis should well covered so infections on the injection site is prevented.
Cycling and Stacking
In designing your Testosterone Phenylpropionate cycle, the major factors are length of cycle, bulking or cutting cycle, and stacking with other steroids. Stacking with steroids can improve the outcome of the medications while making sure effective stacking needs to be compatible in order to reduce side effects.
Coaching Cycle Preparation
In designing the cycle with Testosterone Phenylpropionate, you need to realize there will be an average length of a cycle between 8 weeks to 12 weeks. You need to realize testosterone phenylpropionate has a long ester association, therefore it takes longer to alter than fast acting esters. This will affect the frequency of injections, which are typically recommended to be done twice a week to maintain stable blood levels.
Testosterone-only cycles are popular, especially for new users because they are easier to follow and testosterone has a well-established profile. More experienced users will often run a longer cycle and stack other compounds for synergy.
Bulking cycles: Anabolic steroids such as Nandrolone Phenylpropionate (NPP) are often stacked with testosterone for synergistic effects when gaining muscle mass.
Cutting cycles: To increase leanness, compounds such as Selective Androgen Receptor Modulators (SARMs) could be used with testosterone due to their anabolic activity with a lower risk of side effects than regular anabolic steroids.
Stacking with Other Anabolic Steroids

Stacking Testosterone Phenylpropionate with other anabolic steroids will involve knowledge about the action of each steroid and side effect profile. Below are a few commonly used stacks:
Bulking: Testosterone Phenylpropionate + NPP + Dianabol
Cutting: Testosterone Phenylpropionate + Winstrol + SARMs (Ostarine)
Dosage based on stack will vary, but should always be kept within reasonable and safe dose limits to minimize side effects. Post-Cycle Therapy (PCT) will follow the completion of the cycle as a means of recovering natural homeostasis and keeping your gains.
Side Effects and Risk Management

Testosterone Phenylpropionate is a synthetic anabolic steroid and, therefore, associated risks follow. Proper risk management will involve taking the side effects into account, and will involve a method of reducing the chances of them occurring. Common Side Effects
Common side effects of testosterone phenylpropionate include:
Gynecomastia: Enlarged breast tissue in men due to estrogenic effects.
Hair Loss: Androgenic effects may cause hair thinning and/or male pattern baldness.
Acne: Increased oil production in skin creates acne.
Blood Pressure: High blood pressure due to water and sodium retention.
Cholesterol: Changes in lipid profiles, including LDL cholesterol.
The use of this androgenic steroid, there will be increased estrogen, so all the side effects are predominantly estrogenic in nature. The aromatase enzyme converts testosterone into estrogen and can cause water retention and increased blood pressure.
Minimizing Side Effects
To reduce side effects, the following may help:
Aromatase inhibitors: Prescribed medications that inhibit aromatase from converting testosterone into estrogen.
Lifestyle: Proper diet and exercise can combat blood pressure and cholesterol.
Dosing: Minimizing dosing of testosterone phenylpropionate may mitigate side effects.
Cycling: Short durations of steroid cycles will help mitigate its effects on the body.
Comprehensive blood work pre, post, and during cycling may help monitor your body’s response to the hormone and allow adjustments to protocols to reduce side effects.
Post Cycle Therapy (PCT) and Recovery

Proper hormone levels following cycle is key to maintaining gains and minimizing side effects we want to have an effective post cycle therapy protocol and recovery methods to normalize testosterone levels after ceasing testosterone phenylpropionate.
PCT
Nolvadex and Clomid are the most common medications used in PCT to stimulate natural production of testosterone after steroid cycling.
Nolvadex: General dosing will begin at 20-40mg daily and taper for 4-6 weeks.
Week 1-2: 40mg daily
Week 3-4: 20mg daily
Week 5-6: 10mg daily (as necessary)
Clomid: Staggers in at 50mg daily for 4-6 weeks and then taper down.
Week 1-3: 50mg daily
Week 4-6: 25mg daily
The degree of dosing on the PCT protocol may depend upon the time and dosage of anabolic steroid cycle; the higher doses would need a more aggressive PCT.
Recovery Following a Cycle of Testosterone Phenylpropionate
Recovery involves hormone stabilization and minimizing symptoms associate with low hormone levels.
Symptoms of Low Testosterone: Symptoms may be fatigue, low sex drive, and loss of muscle.
Hormone stabilization: PCT is effective at restoring potential symptoms of having low testosterone.
Timeline for Recovery: Hormone Levels vary as one continues to improve and stabilize after weeks one to four of PCT, and self-monitoring recovery can take a number of months.
Maintaining blood work is important for monitoring recovery. The balance is monitoring activation of your body’s natural testosterone production while preventing estrogenic effects.
Frequently asked questions
1) What is the half-life of testosterone phenylpropionate? Testosterone phenylpropionate has a half-life of around 3 – 4.5 days.
2) What is testosterone phenylpropionate used for? This synthetic androgen ester is mainly intended to treat male hypogonadism, or testosterone replacement therapy (TRT) in men with primary or secondary testosterone deficiency.
3) What is the quickest acting testosterone? The fastest acting testosterone is testosterone acetate followed by testosterone propionate, which both have a half-life of less than one day and about one day, respectively.
4) What is the ideal cycle length? Recommended cycle lengths for testosterone are usually 10-16 weeks for long-ester preparations.
5) Can testosterone cause diarrhea? Testosterone can also cause diarrhea as a side effect, and this will happen when starting treatment, likely due to changes in hormone levels to gastrointestinal motility.