

Anastrozole and Letrozole are both aromatase inhibitors, a class of drugs used primarily in the treatment of breast cancer among postmenopausal women. They operate by inhibiting the enzyme aromatase, which is responsible for converting androgens into estrogens in the body. This reduction in estrogen levels is particularly beneficial in slowing the growth of certain breast cancers that are sensitive to hormones. While Anastrozole and Letrozole share a common mechanism of action and therapeutic goal, there are differences in their chemical structure, metabolism, and clinical efficacy that may influence a physician’s choice between the two.
The comparison of Anastrozole and Letrozole extends beyond their shared purpose. It involves considerations such as the specific patient populations who may benefit from one drug over the other, the long-term effects and potential for secondary prevention, and the management of common adverse reactions. Furthermore, ongoing clinical trials and research continue to uncover nuances in the roles that Anastrozole and Letrozole play in cancer treatment. With breast cancer being a leading cause of cancer-related death among women worldwide, the selection of the appropriate aromatase inhibitor is critical for optimizing patient outcomes.
Quick Summary
- Anastrozole and Letrozole are aromatase inhibitors used to treat hormone-sensitive breast cancer in postmenopausal women.
- They differ in structure, metabolism, and some clinical outcomes, influencing treatment decisions.
- Research and clinical trials continue to refine their uses and management of side effects.
Comparison of Anastrozole and Letrozole
Anastrozole and Letrozole are both aromatase inhibitors used in the treatment of breast cancer. They operate on the same enzyme system but differ in their specific effects and usage details.
Mechanism of Action
Anastrozole and Letrozole target the aromatase enzyme, which is pivotal in the synthesis of estrogen. By inhibiting this enzyme, these drugs reduce estrogen levels in the body, specifically estradiol and estrone, which can promote the growth of hormone-sensitive breast cancer cells.
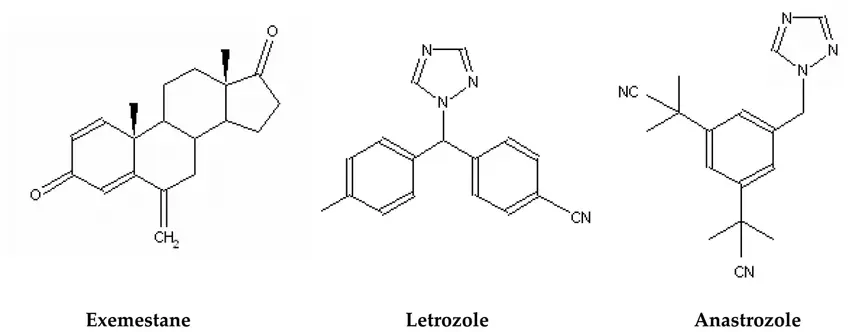
Anastrozole:
- Nonsteroidal inhibitor
- Binds reversibly to the aromatase enzyme
Letrozole:
- Nonsteroidal inhibitor
- Binds more strongly and causes longer suppression of estrogen production
Efficacy in Breast Cancer Treatment
Both anastrozole and letrozole are effective in treating estrogen receptor-positive breast cancer in postmenopausal women.
Studies show:
- Letrozole might provide a slight advantage in terms of efficacy when compared to anastrozole.
- Disease progression is similar under both treatments.
Side Effect Profiles
Although anastrozole and letrozole share many side effects due to their similar mechanism of action, the intensity and occurrence can differ.
Common side effects include:
- Bone pain
- Hot flashes
- Joint pain
- Fatigue
Differences:
- Anastrozole may have a lower incidence of bone fractures compared to letrozole.
- Letrozole might be associated with higher levels of cholesterol compared to anastrozole.
Dosage and Administration
Both medications are administered orally, usually once per day.
Anastrozole:
- Standard dosage: 1 mg
Letrozole:
- Standard dosage: 2.5 mg
Treatment Regimens for Specific Patient Populations

Anastrozole and letrozole are pivotal in treating breast cancer across various patient populations. These medications are selective aromatase inhibitors that reduce estrogen levels, crucial in treating hormone-sensitive breast cancers.
Postmenopausal Women
For postmenopausal women, hormone therapy often incorporates anastrozole or letrozole due to their effectiveness in lowering estrogen levels produced by fat tissue after the ovaries have ceased functioning. Anastrozole is typically prescribed at a dose of 1 mg orally once daily, while letrozole is usually given at 2.5 mg orally once daily. Both medications can be taken with or without food, and their course may last for five to ten years, depending on the clinical assessment of recurrence risk.
- Anastrozole:
- Dosage: 1 mg orally once daily
- Duration: 5-10 years
- Letrozole:
- Dosage: 2.5 mg orally once daily
- Duration: 5-10 years
Premenopausal Women
In premenopausal women with hormone-sensitive breast cancer, the ovaries still produce significant amounts of estrogen. Treatment regimens may combine ovarian suppression with aromatase inhibitors. Letrozole or anastrozole is used in conjunction with medications like goserelin, which suppresses ovarian function. This combination helps to effectively control hormone levels and potentially improves survival outcomes.
- Combined Therapy:
- Aromatase Inhibitor (Anastrozole or Letrozole)
- Ovarian Suppression Agent (e.g., Goserelin)
Men With Breast Cancer
While rare, men with breast cancer, especially those with hormone-sensitive tumors, may benefit from aromatase inhibitors like anastrozole and letrozole. Given that these cancers may be driven by oestrogen, reducing its production through these inhibitors can be a strategic part of the treatment plan. Men generally follow similar dosing protocols as postmenopausal women.
- Treatment Dosing:
- Similar to postmenopausal women
- Specific dose adjustment may be needed under clinical judgment
References
- Anastrozole dosing: https://www.drugs.com/dosage/anastrozole.html
- Letrozole dosing: https://www.drugs.com/dosage/letrozole.html
- Treatment of male breast cancer: https://www.cancer.org/cancer/breast-cancer-in-men/treating/hormone-therapy.html
Long-Term Effects and Secondary Prevention
Long-term management of breast cancer involves understanding the efficacy and secondary impacts of treatments like Anastrozole and Letrozole on recurrence, bone health, and cardiovascular outcomes.
Breast Cancer Recurrence
Anastrozole, marketed as Arimidex, and Letrozole, known as Femara, are aromatase inhibitors commonly prescribed for the prevention of breast cancer recurrence. Both drugs have demonstrated effectiveness in reducing the risk of cancer returning. Studies have shown that Letrozole may reduce the risk slightly more than Anastrozole when used as initial adjuvant therapy.
- Anastrozole: Shown to reduce the chance of recurrence by 40% when compared to placebo.
- Letrozole: Associated with a 43% reduction in the risk of breast cancer return compared to placebo.
Bone Health and Osteoporosis
These aromatase inhibitors may impact bone health leading to osteoporosis and increased fracture risk due to lowered estrogen levels. It is important for patients on these medications to have bone density monitoring and consider supplementation or treatment for bone health.
- Anastrozole: Known to potentially cause a decrease in bone mineral density (BMD).
- Letrozole: Similar to Anastrozole, can result in osteoporosis and heightened fracture risk.
Cardiovascular Health
Both Anastrozole and Letrozole have implications for cardiovascular health, such as potential effects on cholesterol levels. While Letrozole may have a more prominent impact on cardiovascular health, it is crucial for patients to be monitored for any increase in cardiovascular risk during treatment.
- Anastrozole: Linked with a modest increase in cardiovascular events compared to some other therapies.
- Letrozole: Studies suggest an increased incidence of cardiovascular events, hence regular monitoring of heart health is recommended.
References
- Effect of Anastrozole and Tamoxifen as Adjuvant Treatment for Early-Stage Breast Cancer: 10-Year Analysis of the ATAC Trial: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144634/
- Letrozole versus clomiphene for infertility in the polycystic ovary syndrome: https://www.nejm.org/doi/full/10.1056/NEJMoa1313517
- Aromatase inhibitors and bone health in women with breast cancer: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5091079/
Common Adverse Reactions and Management

Anastrozole and Letrozole are medications prescribed for breast cancer treatment and have a profile of side effects that may affect patients. Managing these adverse reactions is crucial for patient quality of life.
General Side Effects
Both Anastrozole, marketed as Arimidex, and Letrozole, known as Femara, commonly cause side effects like hot flashes, joint and muscle pain, fatigue, and headache. Patients may also experience vaginal dryness or irritation, which can cause discomfort.
Anastrozole Side Effects:
- Hot flashes
- Headache
- Joint and muscle pain
- Nausea
Letrozole Side Effects:
- Fatigue
- Bone pain
- Increased cholesterol levels
- Night sweats
Managing Hot Flashes and Night Sweats
To manage hot flashes and night sweats:
- Use layer clothing
- Keep the bedroom cool at night
- Consider prescription medications or natural supplements after consulting a healthcare provider
Endocrine and Reproductive Health
Both drugs can affect endocrine and reproductive health, leading to decreased bone mineral density and an increased risk of osteoporosis. To mitigate these effects, patients may be advised to:
- Supplement with calcium and vitamin D
- Engage in weight-bearing exercises
- Receive bone density scans periodically
Management of Vaginal Dryness/Irritation:
- Use water-based lubricants
- Consult healthcare providers for topical estrogen or other treatments
References
- Anastrozole Side Effects – Drugs.com
- Letrozole Side Effects – Drugs.com
- Managing Aromatase Inhibitor-Associated Bone Loss (AIBL) in postmenopausal women with hormone-sensitive breast cancer: Joint position statement of the International Osteoporosis Foundation, Cancer and Bone Society, and the International Expert Group for AIBL
Clinical Trials and Research on Anastrozole and Letrozole

Anastrozole and letrozole are critical medications in the management of hormone receptor-positive breast cancer, with extensive clinical trials shaping current treatment protocols.
Comparative Studies
Anastrozole (marketed as Arimidex) and letrozole (marketed as Femara) have both been extensively evaluated in clinical trials. A significant trial, the Anastrozole, Tamoxifen, Alone or in Combination (ATAC) trial, demonstrated that anastrozole was more effective than tamoxifen in preventing recurrence of breast cancer. The Lancet reported these pivotal findings:
- Anastrozole reduced the risk of recurrence by 50% compared to tamoxifen.
- 5-year disease-free survival was 84.7% for anastrozole compared to 81.5% for tamoxifen.
Another vital study, the Breast International Group (BIG) 1-98, directly compared letrozole to tamoxifen and found that letrozole significantly improved disease-free survival. Notable points from this trial include:
- Letrozole reduced the risk of breast cancer return by 19% over tamoxifen.
- There was also a 27% lower risk of distant metastasis with letrozole.
Further head-to-head comparisons of anastrozole and letrozole have found similar efficacy between the two, suggesting both are viable first-line therapies in postmenopausal women.
Emerging Therapies and Combinations
Recent research has expanded beyond monotherapy, exploring how anastrozole and letrozole may be used in combination with other drugs. For instance, combining letrozole with palbociclib (Ibrance), a CDK 4/6 inhibitor, has shown promising results in improving progression-free survival in women with HR-positive, HER2-negative advanced breast cancer.
- The addition of palbociclib to letrozole improved median progression-free survival from 14.5 to 27.6 months.
Anastrozole is also part of emerging therapeutic regimens. Research examining the combination of anastrozole with fulvestrant (Faslodex) has demonstrated improved outcomes over anastrozole alone.
- The combination arm had a median progression-free survival increase from 13.5 to 16.6 months compared to anastrozole alone.
On the horizon are examinations of how exemestane (Aromasin), another aromatase inhibitor, fares alongside other contemporary medications such as everolimus (Afinitor). While not as extensively studied in direct comparison to anastrozole or letrozole, exemestane could offer an alternative treatment pathway, particularly in combination therapies.
Clinical trials continue to define the efficacy and safety of these medications, particularly for endometrial cancer, where aromatase inhibitors can be part of the therapeutic arsenal.
Frequently Asked Questions
